
How patient engagement maps to the care journey, what the evidence actually supports, and a vendor-by-vendor breakdown to help healthcare leaders make a confident decision.
Patient engagement has moved from a “nice-to-have” experience layer into a strategic capability that affects access, throughput, communication, safety, loyalty, and — increasingly — reimbursement. HCAHPS scores remain part of the Hospital Value-Based Purchasing framework, missed appointments remain a costly operational drag, and patients increasingly compare their care experience to their banking or retail apps. Choosing the right engagement strategy — and the right mix of platforms — is one of the highest-leverage technology decisions a health system can make.
But patient engagement is not a single product category, and the evidence base is narrower than much vendor marketing suggests. This guide does two things: it frames engagement as a care-journey capability grounded in what the research actually supports, and it gives you a practical, vendor-by-vendor evaluation framework you can bring into an RFP or board presentation. Rather than repeat marketing claims, we tighten the numbers, map the landscape honestly, and show where each category — including the physical care environment — fits.
What Patient Engagement Actually Is
Patient engagement is often discussed as if it were a single product. It is not. In practice, it is the set of workflows, technologies, and environments that help patients and caregivers understand care, participate in decisions, navigate services, complete required tasks, and stay connected before, during, and after an encounter. AHRQ frames this broadly as engaging patients and families in their care; the World Health Organization similarly describes it as building the capacity of patients, families, carers, and providers to support safer, better care.
That distinction matters, because engagement is not the same thing as patient satisfaction, and it is not limited to the patient portal. A portal login, a completed pre-visit questionnaire, a secure message, a bedside education session, a telehealth check-in, a remote-monitoring alert, and a caregiver proxy account are all forms of engagement. The most useful way to understand the market is to classify it by care stage.

Before care is about reducing friction and preparing patients to arrive ready: digital front doors, self-scheduling, reminders, text confirmations, intake forms, benefits communication, e-consent, pre-procedure preparation, and care-gap outreach. The evidence here is relatively strong — systematic reviews find that telephone and SMS reminders improve attendance and reduce missed appointments compared with no reminder, even if effect sizes vary by context. EHR-tethered tools such as MyChart and MEDITECH’s patient-facing products now handle core front-door tasks like scheduling, pre-visit work, virtual visits, messaging, and results access.
During care, engagement shifts from access to comprehension, coordination, and confidence. In inpatient settings that can mean bedside education, digital whiteboards, meal ordering, request routing, family communication, interpreter access, or in-room assistants connected to the EHR. Oneview, for example, positions its connected-care platform and Ovie assistant around patient guidance, request handling, and real-time unit insight, while CipherHealth focuses on rounding, service recovery, and discharge readiness. The lesson is that “during care” engagement is often workflow orchestration, not just content delivery.
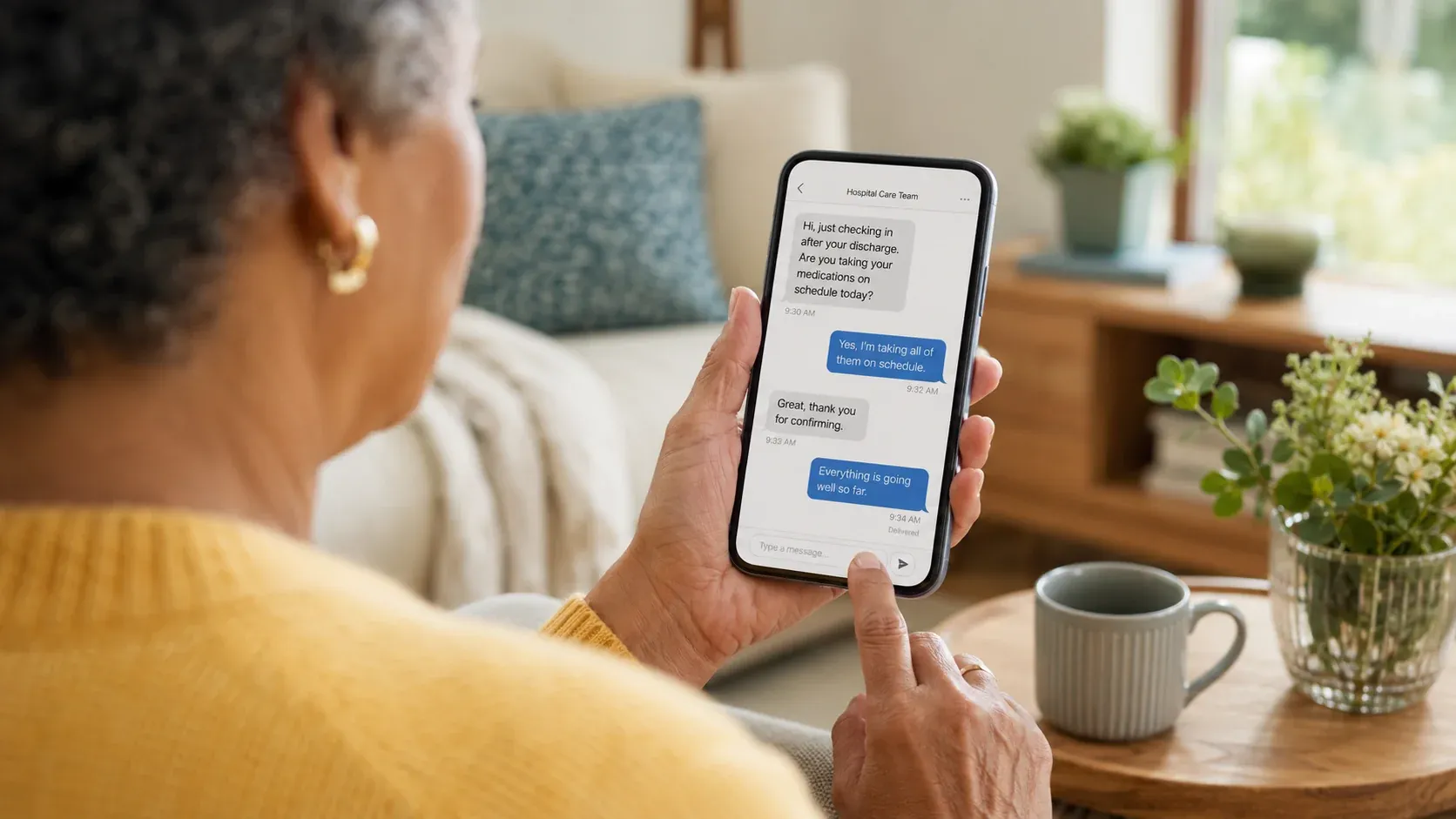
After care is about continuity: discharge instructions, medication support, post-discharge follow-up, secure two-way messaging, patient-reported outcomes, telehealth check-ins, and remote patient monitoring. CMS now broadly covers remote patient monitoring for acute and chronic conditions. AHRQ’s distinction between experience and outcome measures is useful here: a strong post-discharge strategy should measure not just whether a patient liked the communication, but whether they understood instructions, recovered function, controlled symptoms, and avoided preventable escalation.
Why the Stakes Are Higher in 2026
Several forces are converging at once.
Adoption has risen sharply. In 2024, 65% of individuals nationally were both offered and accessed their online medical records or patient portal, up from 25% in 2014, while app-based access rose from 38% in 2020 to 57% in 2024. But access is not the same as use: the same data shows that 87% of individuals encouraged by their provider accessed their portal, versus 57% among those who were not. Engagement is increasingly something health systems design for, not something patients do on their own.
Value-based care keeps experience financially relevant — but be precise about how. HCAHPS sits in the Patient Experience of Care domain within Hospital Value-Based Purchasing, a program CMS funds by reducing participating hospitals’ base operating DRG payments by 2% and redistributing them on performance. Through FY 2026, eight HCAHPS dimensions are included, and the survey structure shifts in later program years. Patient experience materially affects VBP performance — it is a real revenue lever — but it should not be described as “25–30% of all CMS hospital payments.”
Point-solution sprawl is costing more than it saves. Most hospitals still run separate tools for SMS reminders, digital intake, patient education, rounding, and post-discharge follow-up. These disjointed systems create data silos, inconsistent patient experiences, and hidden operational costs in staff time spent reconciling incompatible platforms.
AI has moved from experimental to expected. Predictive outreach, personalized care pathways, conversational scheduling, and real-time sentiment analysis are no longer advanced features — they are baseline expectations for any platform entering a competitive evaluation in 2026. The caution is the one the evidence demands everywhere: a capability in a demo is not the same as an outcome in your workflow.
What the Evidence Actually Supports
The strongest evidence base is narrower than many marketing claims suggest, and a credible buyer keeps the two separate.
Reminders work. Telephone and SMS reminders reliably outperform no reminder for appointment attendance, making them one of the clearest ROI cases in patient engagement. They do not, on their own, guarantee a specific volume lift: self-scheduling, reminder, and rescheduling workflows reduce friction, improve slot utilization, and help fill cancelled appointments, but realized volume impact depends heavily on specialty, staffing, demand, and workflow design. Treat headline figures like “40% more volume” as vendor-specific, not general.
No-shows are a real, variable problem — not a tidy dollar figure. Missed appointments are a substantial operational and financial drag, and no-show rates vary widely by setting, often ranging from roughly 12% to 42% in outpatient studies, with some settings higher. The widely circulated “$150 billion a year” estimate is not cleanly supported by a strong primary source, so we don’t rely on it.

Blended digital education can outperform paper-only approaches — when it’s integrated into clinician workflow. In one JMIR study, patients who received digital education with clinician support reported better understanding, stronger motivation for self-care, greater confidence in decision-making, and stronger intention to follow instructions than patients receiving non-computer-based education. Describe these results precisely: a NICU improvement project, for instance, found that 92% of families highly rated tablet-based discharge teaching and that “prepared for discharge” top-box satisfaction rose from 47% to 70% — which is not the same as a head-to-head “digital vs. paper completion” comparison.
Remote patient monitoring helps in defined settings. A recent systematic review found positive effects on adherence and some safety-related outcomes, though results remain heterogeneous by condition, device, and workflow.
Portals are essential infrastructure, but not a strategy by themselves. Portals are clearly important, yet their impact on utilization and outcomes is more mixed and depends on workflow, clinician adoption, and patient access. “Having a portal” is not the same as having an engagement strategy. Engagement succeeds when content, timing, workflow, staffing, and measurement align around a specific use case — reducing no-shows, improving discharge comprehension, capturing PROMs, or supporting chronic-disease management — an emphasis echoed across AHRQ’s patient-engagement research.
The Core Capabilities to Evaluate
Not all platforms cover the same ground. Some are built primarily for outpatient communication; others focus on inpatient bedside engagement; a few extend into the physical care environment itself. Before comparing vendors, align your team on which capabilities are must-haves versus nice-to-haves for your setting — and weight them against the evidence above.

Interoperability, Privacy, and Equity
Whether engagement tools actually get used often comes down to three things buyers underweight.
Interoperability. ONC’s Cures Act Final Rule was designed to support secure access, exchange, and use of electronic health information and to expand standards-based (FHIR) APIs; CMS’s interoperability policies rely on similar FHIR-based access. Insist on bidirectional integration with your specific EHR — not “Epic-compatible” marketing — and confirm exactly what writes back to the chart.
Privacy and consent. Under HIPAA, covered entities and business associates must protect electronic protected health information with administrative, physical, and technical safeguards. Just as important — and often missed — information a patient directs to a third-party consumer app may no longer be protected by HIPAA if that app is neither a covered entity nor a business associate. In Europe, the GDPR treats health data as a special category subject to specific processing conditions, and the European Health Data Space adds health-specific rules for access, control, and cross-border exchange. If your engagement stack hands data to consumer apps, your consent language needs to say so plainly.

Equity and accessibility — designed in, not bolted on. Portal and digital-engagement use remain uneven by age, race and ethnicity, language, literacy, and disability. The same ONC data that shows rising adoption also shows that provider encouragement materially changes uptake — 87% of encouraged individuals accessed their portal versus 57% of those not encouraged — and that proxy or caregiver access more than doubled between 2020 and 2024. MEDITECH’s patient tools, for example, emphasize assistive-technology support and inclusive design. The implication is straightforward: if you want engagement, design for caregivers, language access, disability access, and supported onboarding from day one.
Measuring Whether It’s Working: KPIs, PREMs, and PROMs
Platforms are easy to buy and hard to evaluate post-implementation. Define your success metrics before you sign — and make sure the platform’s analytics layer can surface them without a custom export request.
Start by separating measures that are routinely conflated. AHRQ distinguishes patient-reported experience measures (PREMs) — did the visit go well? — from patient-reported outcome measures (PROMs) — did the patient get better? HCAHPS is a standardized experience survey tied to reimbursement, and patient activation measures something different again. They are all useful, but collapsing them into one vague idea of “engagement” produces dashboards that look busy and decide nothing. The operational KPIs below sit alongside — not instead of — those patient-reported measures.
| Metric | What It Measures | Why It Matters |
|---|---|---|
| SMS Reply Rate | Active patient participation in outreach | Low reply rate signals content quality or timing problems before they show up in HCAHPS |
| Video Completion Rate | Education content engagement depth | Completion correlates with improved medication adherence and discharge readiness |
| No-Show Rate by Outreach Method | Channel effectiveness for scheduling adherence | Reveals which communication channel actually changes behavior for your population |
| Reach Rate vs. Response Rate Gap | Messaging quality vs. delivery infrastructure | High reach + low response = messaging content or CTA problem, not a technical one |
| HCAHPS Discharge Domain Score | Patient-reported understanding of discharge instructions | Tied to Hospital VBP performance; lowest-scoring domain in many health systems |
| Education Charting Rate | % of patient education automatically written to the EHR | Manual charting = staff burden + data gaps; auto-charting measures real platform integration depth |
| 30-Day Readmission Rate | Post-discharge care plan adherence | Leading indicator of both clinical and platform effectiveness; tracked by CMS |
Solution Categories at a Glance
Before naming vendors, it helps to see the categories side by side. No single category “wins” — each solves a different problem at a different moment in the journey, and most health systems end up running several.
| Category | What it does | Representative vendors | Best-fit use cases | Watch-outs |
|---|---|---|---|---|
| EHR-tethered portal & app | Results, scheduling, billing, messaging, proxy access, telehealth entry, records sharing | Epic MyChart; MEDITECH portal / MyHealth | Scheduling, results, messaging, caregiver access, virtual follow-up | Often fragmented across organizations; value depends on activation and clinician use |
| Outreach & care coordination | Reminders, pre-care outreach, care-gap closure, discharge calls, escalation | CipherHealth; GetWell Navigate | No-show reduction, discharge follow-up, care-gap outreach, service recovery | Needs tight workflow ownership; adds another comms layer if poorly integrated |
| In-room bedside / connected care | Bedside education, request routing, self-service, digital whiteboards, staff workflow support | Oneview; GetWell point-of-care | Inpatient education, family communication, requests, care-team support | Depends on room infrastructure, change management, and nursing workflow |
| Telehealth & hybrid care | Video visits, asynchronous messaging, virtual triage, follow-up | Portal / EHR plus health-system telehealth | Chronic-disease follow-up, behavioral health, post-discharge touchpoints | Safety, equity, and reimbursement rules keep evolving |
| RPM & RTM | Device setup, home data capture, monitoring, escalation, treatment management | EHR-linked and dedicated monitoring programs | Hypertension, diabetes, heart failure, rehab adherence, post-acute | Not universal; depends on staffing, billing, and device adherence |
| Experiential & environmental | Visible education, sensory interaction, calming content, waiting-room engagement, space analytics | Ouva | Waiting rooms, pediatric lobbies, de-escalation zones, facility messaging, orientation | Complements — does not replace — portal, outreach, or clinical monitoring |
This view synthesizes official product pages and public guidance for MyChart, MEDITECH, GetWell, Oneview, CipherHealth, CMS RPM policy, and Ouva. The “best-fit” and “watch-outs” columns are our analysis, not vendor claims.
Vendor Landscape: A Detailed Comparison
The patient engagement market in 2026 spans everything from point-solution texting tools to full-scale interactive patient care systems. Below is an honest look at the leading platforms, organized by their primary architecture and use case.
GetWell (formerly GetWellNetwork)
Inpatient-first platform

GetWell is one of the most widely deployed interactive patient care platforms in the U.S.; current company materials describe serving more than 10 million patients a year across 1,000+ hospitals and clinical partner sites. Its flagship GetWell Inpatient solution uses bedside TVs and tablets to deliver condition-specific education, service requests, and Patient Pathways — structured digital care plans that walk patients through their stay. GetWell Navigate extends this with AI-driven conversational texting for outpatient and post-discharge follow-up.
Strengths
- Deep Epic and Oracle Health integration with automatic chart write-back
- Proven at scale — 10M+ patients a year across 1,000+ hospitals and partner sites
- Patient Pathways feature is highly configurable per service line
- GetWell Rounds+ enables structured digital rounding
- GetWell Navigate delivers AI texting at population-health scale
Oneview Healthcare
Inpatient-first platform

Oneview operates as a cloud-native, connected-care platform focused on the inpatient “care experience.” It runs on dedicated touchscreen devices and hospital TVs to deliver patient self-service — meal ordering, room controls, entertainment, and condition-specific education. Its Ovie AI software layer adds conversational patient guidance that runs on existing room hardware and connects to clinical systems to handle service requests. Oneview operates internationally across North America, Australia, and Europe.
Strengths
- Cloud-native architecture enables enterprise-wide scaling
- Strong patient self-service can reduce nurse call volume
- Interactive analytics dashboards for unit and experience insight
- Ovie AI runs on existing room hardware — no new device required
- Track record with multi-site health system deployments
CipherHealth
Rounding & outreach specialist

CipherHealth has carved a strong niche in two specific workflows: digital rounding and automated outreach. CipherRounds enables structured, real-time patient rounds with immediate feedback capture and issue escalation. CipherOutreach automates post-discharge follow-up via calls, texts, and email — integrated directly with Epic to surface patient responses within the clinical workflow without manual intervention. Health systems using CipherHealth commonly report HCAHPS improvement and readmission reduction as primary outcomes.
Strengths
- Best-in-class digital rounding with real-time service recovery workflows
- Seamless Epic integration — responses auto-surface in the EHR
- Strong post-discharge outreach automation with clinical escalation logic
- Clear ROI story: widely cited HCAHPS improvement case studies
- Relatively fast implementation compared to full inpatient systems
Epic MyChart
Portal-based engagement

MyChart is not sold as a standalone product — it is the patient engagement layer bundled with Epic EHR implementations. For health systems already on Epic, it offers the deepest possible data integration: appointment scheduling, pre-visit questionnaires, secure messaging, billing, and a growing set of AI-powered features like visit summaries and care gap notifications. It reaches patients through a mobile app with push notifications, making it arguably the most widely used patient engagement tool in U.S. healthcare by sheer installed base.
Strengths
- Zero integration risk for Epic health systems — native data access
- High patient adoption due to existing familiarity and Epic’s market share
- Continuously expanding AI features (visit summaries, care gap outreach)
- Appointment scheduling and pre-visit intake are extremely polished
- No additional per-patient licensing cost for Epic health systems
MEDITECH Expanse Patient Engagement
EHR-bundled
MEDITECH’s patient engagement tools are bundled within its Expanse EHR platform, targeting community hospitals and critical access facilities that may not have the budget or IT infrastructure for an Epic-scale implementation. It covers telehealth, secure bidirectional SMS, appointment reminders, pre-visit questionnaires, and patient portal access. Adaptive device and assistive-technology support addresses accessibility requirements that many competitors overlook.
Strengths
- Strong value proposition for community hospitals already on MEDITECH
- Solid accessibility and adaptive device support
- Telehealth integration within the same workflow as in-person care
- Competitive total cost of ownership for mid-market health systems
The Gap Most Platforms Don’t Fill: Physical-Environment Engagement
Across the mainstream platforms above, three capabilities are consistently missing — sensory environments, behavioral health de-escalation, and specialty therapy support. This isn’t a minor feature gap; it’s a category gap that leaves hospitals managing some of their highest-acuity patient populations with the same passive TV screens they’ve had for decades.
The case for active environmental engagement is growing. Patients in behavioral health units who experience prolonged agitation have worse clinical outcomes and drive higher pharmacological intervention rates. Patients with autism spectrum disorder (ASD) in waiting rooms or procedural spaces face a near-total absence of clinically appropriate engagement tools. And the general waiting room — where most patients form their first impression of a health system — remains largely passive, even in facilities that have invested heavily in digital front-door tools.

What Active Environment Engagement Actually Looks Like
The most effective ambient engagement systems share several characteristics: they are touch-optional (important for infection control and patients with limited mobility), they adapt in real time to patient presence and behavior, and they integrate clinical content — condition education, procedure walkthroughs, calming exercises — directly into the physical environment rather than requiring patients to pull out a device.
Interactive displays that respond to gesture and movement, AI-driven soundscapes that shift with patient state, and cause-and-effect therapy exercises that sustain attention for neurodivergent patients are categorically different from a bedside entertainment system or a patient portal. They address engagement for patients who may not be able or willing to use a smartphone or tablet at all.

Ouva’s strongest fit is as a physical-space engagement and education layer — not a replacement for portals, outreach, or RPM. Its product and case-study pages emphasize device-agnostic deployment on existing PCs, TVs, and tablets, optional dedicated stations or large-format video walls, and engagement analytics for waiting rooms, patient rooms, pediatric spaces, and behavioral-health-adjacent de-escalation zones. The more useful frame is a layered engagement architecture: portals and apps handle records, scheduling, and secure messaging; outreach platforms handle follow-up; telehealth and RPM extend care into the home; and an environmental layer handles waiting, orienting, calming, and visible communication inside the building itself.
Ouva runs on existing hospital screens and projectors to create those interactive sensory environments without requiring proprietary hardware. It’s worth evaluating alongside the mainstream platforms if your health system includes any of these care settings. Case studies from facilities like Piedmont Children’s Hospital and Kaiser Permanente illustrate the clinical use cases in practice.
Evaluation Checklist for CIOs and Hospital Administrators
Use this framework to structure vendor demonstrations, score RFP responses, and build your internal business case. Assign each item a weight based on your organization’s specific priorities.
Architecture & Integration
- Bidirectional EHR integration confirmed with your specific EHR (not just “Epic-compatible” marketing)
- Auto-charting of patient education completion, survey responses, and care plan interactions
- Hardware-agnostic deployment — no mandatory proprietary device purchase
- Cloud-native architecture with documented uptime SLAs and disaster recovery
- HIPAA-compliant data handling with a signed BAA, documented breach history, and clear terms for any data shared with third-party or consumer apps
Patient Communication & Education
- True omnichannel: SMS, email, voice, push — with channel preference stored per patient
- Clinically validated education library with condition-specific and procedure-specific content
- Visual-first content formats for low-health-literacy populations
- Discharge education automation triggered at point of discharge, with follow-up logic
- Ability to A/B test message content and timing from the admin dashboard
AI & Personalization
- AI-driven outreach personalization based on patient risk profile, history, and behavior
- Predictive risk scoring that triggers escalation before a patient calls or no-shows
- Natural language processing for conversational patient interactions at scale
- AI outputs are explainable to clinical staff — not a black box
Analytics & Performance Management
- Role-based dashboards: executive, unit manager, and clinical staff views
- HCAHPS domain tracking by unit, admission type, and engagement level
- PREM, PROM, and HCAHPS tracking kept distinct — not collapsed into a single “engagement” score
- Reach rate vs. response rate segmentation to diagnose messaging failures
- No-show rate tracking by outreach method and patient segment
- Data export in standard formats (CSV, HL7, FHIR) without additional fees
Special Populations & Physical Environments
- Engagement options for patients who cannot use mobile devices (pediatric, geriatric, behavioral health)
- Waiting room and lobby engagement tools — not just bedside or mobile
- Behavioral health de-escalation or calming environment capabilities
- ASD-appropriate therapy engagement if applicable to your service lines
- Accessibility: screen reader support, adjustable font sizes, caregiver/proxy access, and multilingual content
Implementation & Support
- Reference customers at comparable health systems willing to speak directly
- Time-to-deployment estimate with realistic assumptions — not best-case scenarios
- Defined process for ongoing content updates and platform configuration changes
- Contractual SLA for support response times, including after-hours critical issues
- Clear roadmap for AI and feature development over the next 18–24 months
How to Choose: Matching Platform to Priority
No single platform dominates every use case. The most useful question is not “which platform does everything?” It’s “which engagement problem are we solving, for which population, at which moment in the journey, and how will we measure success?” The right choice depends on your primary problem, your existing EHR, your patient population mix, and your capital-versus-operational budget constraints.
- If your primary gap is post-discharge readmissions and follow-up: CipherHealth’s rounding and outreach tools have a strong evidence base and fast time-to-ROI for this specific outcome.
- If you’re on Epic and need better patient communication without adding a new vendor: Maximize MyChart first. Its native integration and AI roadmap are improving rapidly, and you’re likely underutilizing what’s already licensed.
- If you need full inpatient engagement — education, service requests, entertainment, and rounding — in one system: GetWell and Oneview are the mature options, each with a distinct architecture philosophy. GetWell favors software configurability; Oneview leans toward cloud-native scalability.
- If you have specialty care settings — pediatric, behavioral health, ASD therapy — where standard platforms leave significant gaps: Evaluate dedicated environment engagement tools alongside your primary platform rather than assuming your main vendor will cover these populations adequately.
Whatever you choose, two things are true at once. Vendor sprawl is real — disjointed experiences, siloed analytics, and staff time lost reconciling incompatible systems are expensive in a value-based environment, so favor fewer, well-integrated systems. And no single platform covers every moment of the journey, so the goal is a coherent, layered architecture matched to your priorities: portals and apps for records and scheduling, outreach for follow-up, telehealth and RPM for the home, and an environmental layer for the moments inside your walls that the others miss.
Start with clear KPIs, honest RFP questions, and reference conversations with peer institutions — and you’ll be in a strong position to make a decision that serves both your patients and your balance sheet.
Related Reading
Interactive Patient Education: Boosting Patient Engagement
Learn how modern hospitals are leveraging interactive patient education and emotion-aware AI to boost patient engagement, reduce stays, and enhance recovery.

Patient Education for Hospitals: Interactive & AI Care
Discover how interactive patient education solutions for hospitals improve outcomes. Learn how AI companions and gamification reduce stress and increase adherence.

Interactive Sensory Walls for Autism (ASD) & Therapy
Discover how AI-powered interactive sensory walls are transforming autism therapy by providing personalized, engaging, and adaptive sensory experiences.